
Efficacy of Barhemsys
A Broadly Studied and Proven Antiemetic Treatment
Barhemsys was studied in 4 pivotal trials encompassing ~2000 patients.1
Barhemsys 10 mg as a Rescue Treatment for PONV
Studied in Patients Who Failed Prophylaxis
Barhemsys 10 mg was evaluated for the rescue treatment of PONV in a randomized, double-blind, placebo-controlled, multicenter trial comprising adult patients who had undergone elective ambulatory or inpatient surgery under general anesthesia and failed prior antiemetic prophylaxis with 1 or more agents of a different class (N=465).1,2,*
Prophylactic Agents Used
| Placebo (n=235) |
Barhemsys 10 mg (n=230) |
|
|---|---|---|
| 5-HT3 antagonist | 77.4% | 76.5% |
| Dexamethasone | 61.7% | 67.8% |
| Other | 8.9% | 12.2% |
Number of Prophylactic Agents
| Placebo (n=235) |
Barhemsys 10 mg (n=230) |
|
|---|---|---|
| 1 antiemetic | 51.1% | 52.6% |
| 2 antiemetics | 40.9% | 39.6% |
| ≥3 antiemetics | 5.1% | 7.8% |
Qualifying PONV Event
| Placebo (n=235) |
Barhemsys 10 mg (n=230) |
|
|---|---|---|
| Emesis | 24.3% | 17.4% |
| Nausea | 97.0% | 99.1% |
| Mean ± SD nausea score | 6.2 ± 2.2 | 6.3 ± 2.3 |
| Occurrence in PACU | 73.2% | 73.5% |
| Occurrence 0-2 hours after surgery | 71.9% | 67.8% |
*Total IV anesthesia with propofol was not permitted, though a single dose at induction was allowed.
Barhemsys 10 mg: Proven Effective for Your Patients With Breakthrough PONV After Failed Prophylaxis
At 24 hours
29%
Placebo
(n=235)
42%
Barhemsys 10 mg
(n=235)
10mg
In patients who failed prophylaxis
42% (96/230) of Barhemsys 10 mg-treated patients met the criteria for complete response at 24 hours compared with 29% (67/235) of placebo-treated patients1,2,†
Difference (95% CI): 13% (5%, 22%); P=0.003
The primary efficacy endpoint was complete response, defined as absence of any episode of emesis (vomiting or retching) or use of rescue medication within the first 24 hours after treatment, excluding emesis in the first 30 minutes.1,2
†The primary efficacy analysis was performed with the modified intention-to-treat population (randomized patients who received study medication).
Kaplan-Meier Curves: Complete Response Over Time2,‡
Try adjusting the slider to take a closer look at the time points.
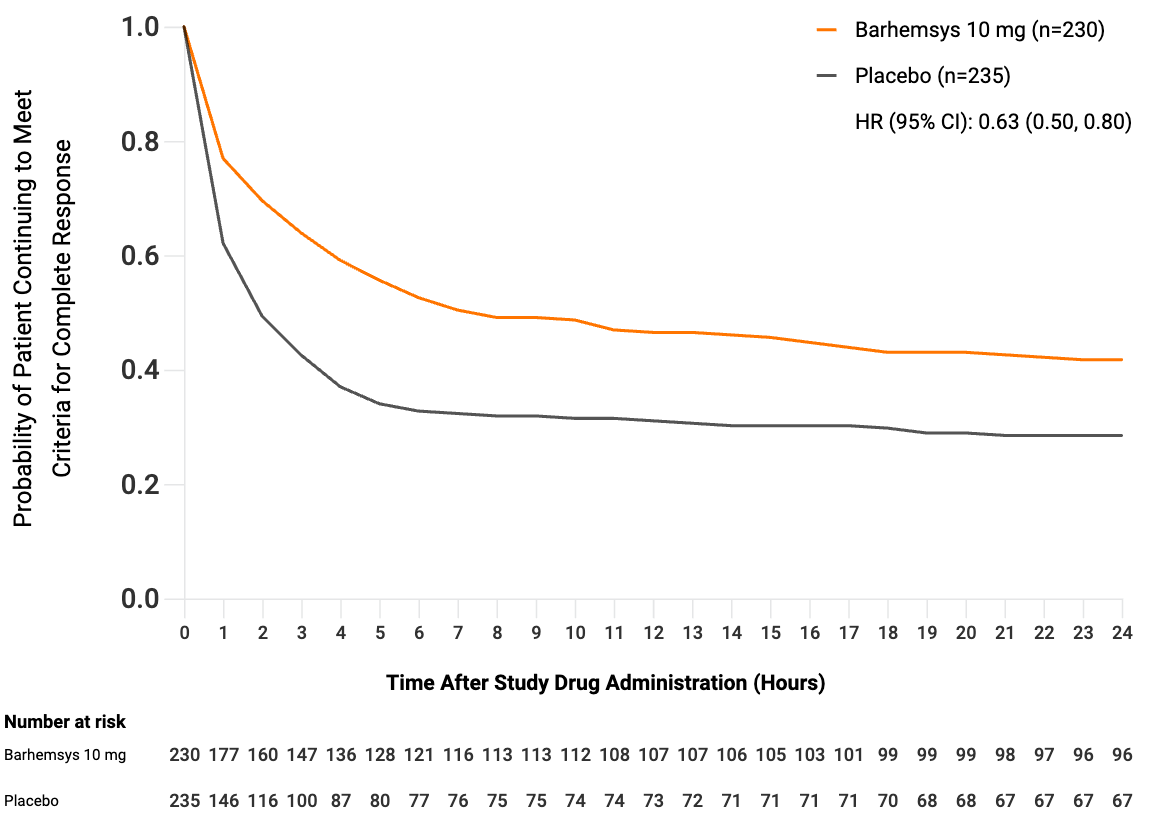
‡The secondary endpoints listed were prespecified. These endpoints were not adequately powered nor error controlled, and observed treatment differences cannot be regarded as statistically significant.
Complete Response Rates at Prespecified Times
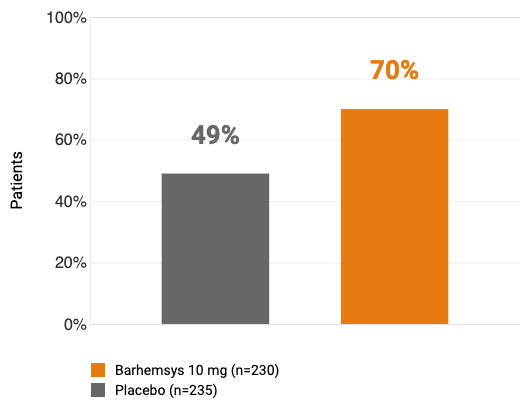
Secondary endpoint
In patients who failed prophylaxis
70% (160/230) of patients met the criteria for complete response at 2 hours after receiving a 10 mg dose of Barhemsys compared with 49% (116/235) of placebo-treated patients2,§
At each of the prespecified interim time points (4 and 6 hours), the percentage of patients who met the criteria for complete response was approximately 20% higher with Barhemsys 10 mg compared with placebo.2
§The secondary endpoint was not adequately powered nor error controlled, and observed treatment differences cannot be regarded as statistically significant.
Secondary Endpoint: PACU and Hospital Length of Stay
In patients who failed prophylaxis, Barhemsys 10 mg-treated patients had 35 minutes shorter PACU LOS and 6 hours shorter mean hospital LOS than placebo-treated patients.2,||
||The secondary endpoints were prespecified. These endpoints were not adequately powered nor error controlled, and observed treatment differences cannot be regarded as statistically significant.
Barhemsys 5 mg Is Part of a Proven Combination Prophylaxis Therapy
Studied in High-Risk Patients
Barhemsys 5 mg was evaluated in combination with an antiemetic of a different class for the prevention of PONV in a randomized, double-blind, placebo-controlled, multicenter trial comprising adult patients at high risk of developing PONV undergoing general anesthesia during elective inpatient surgery (N=1147).1,3,*
Patient Baseline Characteristics at Randomization
Characteristics
| Placebo + Another Antiemetic (n=575) |
Barhemsys 5 mg + Another Antiemetic (n=572) |
|
| Age, mean (SD) | 48 (14) | 49 (14) |
| Sex, % female | 96.9% | 96.5% |
Baseline PONV Risk
| Placebo + Another Antiemetic (n=575) |
Barhemsys 5 mg + Another Antiemetic (n=572) |
|
| 2 risk factors | 0.2% | 0.2% |
| 3 risk factors | 56.7% | 56.1% |
| 4 risk factors | 43.8% | 43.7% |
Other Antiemetic Agent Used
| Placebo + Another Antiemetic (n=575) |
Barhemsys 5 mg + Another Antiemetic (n=572) |
|
| Ondansetron | 51.1% | 49.8% |
| Dexamethasone | 43.8% | 46.5% |
| Other | 3.7% | 2.3% |
*Total IV anesthesia with propofol was not permitted, though a single dose at induction was allowed. Only nondopaminergic antiemetics were allowed.
Barhemsys 5 mg Demonstrated Efficacy as Part of a Combination Prophylaxis for the Prevention of PONV in High-Risk Patients
At 24 hours
47%
Placebo
+ Another Antiemetic (n=575)
58%
Barhemsys 5 mg
+ Another Antiemetic (n=572)
5mg
In patients who received combination prophylaxis
58% (330/572) of Barhemsys 5 mg-treated patients met the criteria for complete response at 24 hours compared with 47% (268/575) of placebo-treated patients1,3,†
Difference (95% CI): 11% (5%, 17%); P<0.001
Barhemsys as a PONV therapy choice supports the guideline recommendation that adults who are at a high risk for PONV should receive combination prophylactic therapy.1,3,4
The primary efficacy endpoint was complete response, defined as absence of any episode of emesis (vomiting or retching) or use of rescue medication within the first 24 hours following surgery.1,3
†The primary efficacy analysis was performed with the modified intention-to-treat population (randomized patients who received study medication).
Barhemsys as a Prophylactic Monotherapy
Study Design
Barhemsys 5 mg was evaluated as a prophylactic monotherapy for PONV in a randomized, double-blind, placebo-controlled, multicenter trial comprising adult patients at moderate to high risk of developing PONV undergoing general anesthesia and elective surgery (N=342).1,5,*
*Total IV anesthesia with propofol was not permitted, though a single dose at induction was allowed.
Barhemsys Demonstrated Efficacy as a Monotherapy Prophylaxis for the Prevention of PONV in Moderate- to High-Risk Patients
At 24 hours
33%
Placebo
(n=166)
44%
Barhemsys 5 mg
(n=176)
5mg
In patients who received monotherapy prophylaxis
44% (78/176) of Barhemsys 5 mg-treated patients met the criteria for complete response at 24 hours compared with 33% (54/166) of placebo-treated patients1,5,†
Difference (95% CI): 12% (2%, 22%); P=0.033
Barhemsys demonstrated single-agent efficacy when compared with placebo.1,5
The primary efficacy endpoint was complete response, defined as absence of any episode of emesis (vomiting or retching) or use of rescue medication within the first 24 hours following surgery.1,5
†The primary efficacy analysis was performed with the modified intention-to-treat population (randomized patients who received study medication).
‡Difference in outcomes between the control and treatment group was calculated with complete response results to the tenths and rounded to the nearest whole number.
Indications
Barhemsys is a selective dopamine-2 (D2) and dopamine-3 (D3) receptor antagonist indicated in adults for:
- prevention of postoperative nausea and vomiting (PONV), either alone or in combination with an antiemetic of a different class
- treatment of PONV in patients who have received antiemetic prophylaxis with an agent of a different class or have not received prophylaxis
Important Safety Information
Contraindication
Barhemsys is contraindicated in patients with known hypersensitivity to amisulpride.
QT Prolongation
Barhemsys causes dose- and concentration-dependent prolongation of the QT interval. The recommended dosage is 5 mg or 10 mg as a single intravenous (IV) dose infused over 1 to 2 minutes.
Avoid Barhemsys in patients with congenital long QT syndrome and in patients taking droperidol.
Electrocardiogram (ECG) monitoring is recommended in patients with pre-existing arrhythmias/cardiac conduction disorders, electrolyte abnormalities (e.g., hypokalemia or hypomagnesemia), congestive heart failure, and in patients taking other medicinal products (e.g., ondansetron) or with other medical conditions known to prolong the QT interval.
Adverse Reactions
Common adverse reactions reported in ≥ 2% of adult patients who received Barhemsys 5 mg (N=748) and at a higher rate than placebo (N=741) in clinical trials for the prevention of PONV were: chills (4% vs. 3%), hypokalemia (4% vs. 2%), procedural hypotension (3% vs. 2%), and abdominal distention (2% vs. 1%).
Serum prolactin concentrations were measured in one prophylaxis study where 5% (9/176) of Barhemsys-treated patients had increased blood prolactin reported as an adverse reaction compared with 1% (1/166) of placebo-treated patients.
The most common adverse reaction, reported in ≥ 2% of adult patients who received Barhemsys 10 mg (N=418) and at a higher rate than placebo (N=416), in clinical trials for the treatment of PONV was infusion site pain (6% vs. 4%).
Use in Specific Populations
Pregnancy
Available data with amisulpride use in pregnant women are insufficient to establish a drug associated risk of major birth defects, miscarriage or adverse maternal or fetal outcomes.
Lactation
Amisulpride is present in human milk. There are no reports of adverse effects on the breastfed child and no information on the effects of amisulpride on milk production.
Barhemsys may result in an increase in serum prolactin levels, which may lead to a reversible increase in maternal milk production. In a clinical trial, serum prolactin concentrations in females (n=112) increased from a mean of 10 ng/mL at baseline to 32 ng/mL after Barhemsys treatment and from 10 ng/mL to 19 ng/mL in males (n=61). No clinical consequences due to elevated prolactin levels were reported.
To minimize exposure to a breastfed infant, lactating women may consider interrupting breastfeeding and pumping and discarding breast milk for 48 hours after receiving a dose of Barhemsys.
Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
Geriatric Use
No overall differences in safety or effectiveness were observed between these patients and younger patients, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
Drug Interactions
- Barhemsys causes dose- and concentration-dependent QT prolongation. To avoid potential additive effects, avoid use of Barhemsys in patients taking droperidol.
- ECG monitoring is recommended in patients taking other drugs known to prolong the QT interval (e.g., ondansetron).
- Reciprocal antagonism of effects occurs between dopamine agonists (e.g., levodopa) and Barhemsys. Avoid using levodopa with Barhemsys.
To report SUSPECTED ADVERSE REACTIONS, contact Acacia Pharma at 1-877-357-9237 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Please click to access full Prescribing Information.
BAR HCP ISI 09/2022
Indication
Barhemsys is a selective dopamine-2 (D2) and dopamine-3 (D3) receptor antagonist indicated in adults for:
- prevention of postoperative nausea and vomiting (PONV), either alone or in combination with an antiemetic of a different class
- treatment of PONV in patients who have received antiemetic prophylaxis with an agent of a different class or have not received prophylaxis
Important Safety Information
Contraindication
Barhemsys is contraindicated in patients with known hypersensitivity to amisulpride.
QT Prolongation
Barhemsys causes dose- and concentration-dependent prolongation of the QT interval. The recommended dosage is 5 mg or 10 mg as a single intravenous (IV) dose infused over 1 to 2 minutes.
Avoid Barhemsys in patients with congenital long QT syndrome and in patients taking droperidol.
Electrocardiogram (ECG) monitoring is recommended in patients with pre-existing arrhythmias/cardiac conduction disorders, electrolyte abnormalities (e.g., hypokalemia or hypomagnesemia), congestive heart failure, and in patients taking other medicinal products (e.g., ondansetron) or with other medical conditions known to prolong the QT interval.
Adverse Reactions
Common adverse reactions reported in ≥ 2% of adult patients who received Barhemsys 5 mg (N=748) and at a higher rate than placebo (N=741) in clinical trials for the prevention of PONV were: chills (4% vs. 3%), hypokalemia (4% vs. 2%), procedural hypotension (3% vs. 2%), and abdominal distention (2% vs. 1%).
Serum prolactin concentrations were measured in one prophylaxis study where 5% (9/176) of Barhemsys-treated patients had increased blood prolactin reported as an adverse reaction compared with 1% (1/166) of placebo-treated patients.
The most common adverse reaction, reported in ≥ 2% of adult patients who received Barhemsys 10 mg (N=418) and at a higher rate than placebo (N=416), in clinical trials for the treatment of PONV was infusion site pain (6% vs. 4%).
Use in Specific Populations
Pregnancy
Available data with amisulpride use in pregnant women are insufficient to establish a drug associated risk of major birth defects, miscarriage or adverse maternal or fetal outcomes.
Lactation
Amisulpride is present in human milk. There are no reports of adverse effects on the breastfed child and no information on the effects of amisulpride on milk production.
Barhemsys may result in an increase in serum prolactin levels, which may lead to a reversible increase in maternal milk production. In a clinical trial, serum prolactin concentrations in females (n=112) increased from a mean of 10 ng/mL at baseline to 32 ng/mL after Barhemsys treatment and from 10 ng/mL to 19 ng/mL in males (n=61). No clinical consequences due to elevated prolactin levels were reported.
To minimize exposure to a breastfed infant, lactating women may consider interrupting breastfeeding and pumping and discarding breast milk for 48 hours after receiving a dose of Barhemsys.
Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
Geriatric Use
No overall differences in safety or effectiveness were observed between these patients and younger patients, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
Drug Interactions
- Barhemsys causes dose- and concentration-dependent QT prolongation. To avoid potential additive effects, avoid use of Barhemsys in patients taking droperidol.
- ECG monitoring is recommended in patients taking other drugs known to prolong the QT interval (e.g., ondansetron).
- Reciprocal antagonism of effects occurs between dopamine agonists (e.g., levodopa) and Barhemsys. Avoid using levodopa with Barhemsys.
To report SUSPECTED ADVERSE REACTIONS, contact Acacia Pharma at 1-877-357-9237 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Please click to access full Prescribing Information.
BAR HCP ISI 09/2022
5-HT3=serotonin. CI=confidence interval. IV=intravenous. PONV=postoperative nausea and vomiting. SD=standard deviation.
References: 1. Barhemsys [package insert], Indianapolis, IN: Acacia Pharma Inc; 2022. 2. Habib AS, Kranke P, Bergese SD, et al. Amisulpride for the rescue treatment of postoperative nausea or vomiting in patients failing prophylaxis: a randomized, placebo-controlled phase III trial. Anesthesiology. 2019;130(2):203-212. 3. Kranke P, Bergese SD, Minkowitz HS, et al. Amisulpride prevents postoperative nausea and vomiting in patients at high risk: a randomized, double-blind, placebo-controlled trial. Anesthesiology. 2018;128(6):1099-110. 4. Gan TJ, Belani KG, Bergese S, et al. Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesth Analg. 2020;131(2):411-448. 5. Gan TJ, Kranke P, Minkowitz HS, et al. Intravenous amisulpride for the prevention of postoperative nausea and vomiting: two concurrent, randomized, double-blind, placebo-controlled trials. Anesthesiology. 2017;126(2):268-2756. 6. Candiotti KA, Kranke P, Bergese SD, et al. Randomized, double-blind, placebo-controlled study of intravenous amisulpride as treatment of established postoperative nausea and vomiting in patients who have had no prior prophylaxis. Anesth Analg. 2019;128(6):1098-1105.